


 Sign Out
Sign Out




The overall safety profile of empagliflozin plus metformin for patients enrolled in the EMPA-REG OUTCOME study was comparable to the previously known safety profile.
Placebo controlled double-blind trials of 18 to 24 weeks of exposure included 3456 patients, of which 1271 were treated with empagliflozin 10 mg plus metformin and 1259 with empagliflozin 25 mg plus metformin.
The most frequently reported adverse event in clinical trials was hypoglycaemia, which depended on the type of background therapy used in the respective studies (Table 16).
No additional side effects were identified in clinical trials with empagliflozin plus metformin compared to the side effects of the single components.
Tabulated list of adverse reactions: The adverse reactions are listed by absolute frequency. Frequencies are defined as very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), or very rare (<1/10,000), and not known (cannot be estimated from the available data). (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: The frequencies as follows are calculated for adverse reactions regardless of causality.
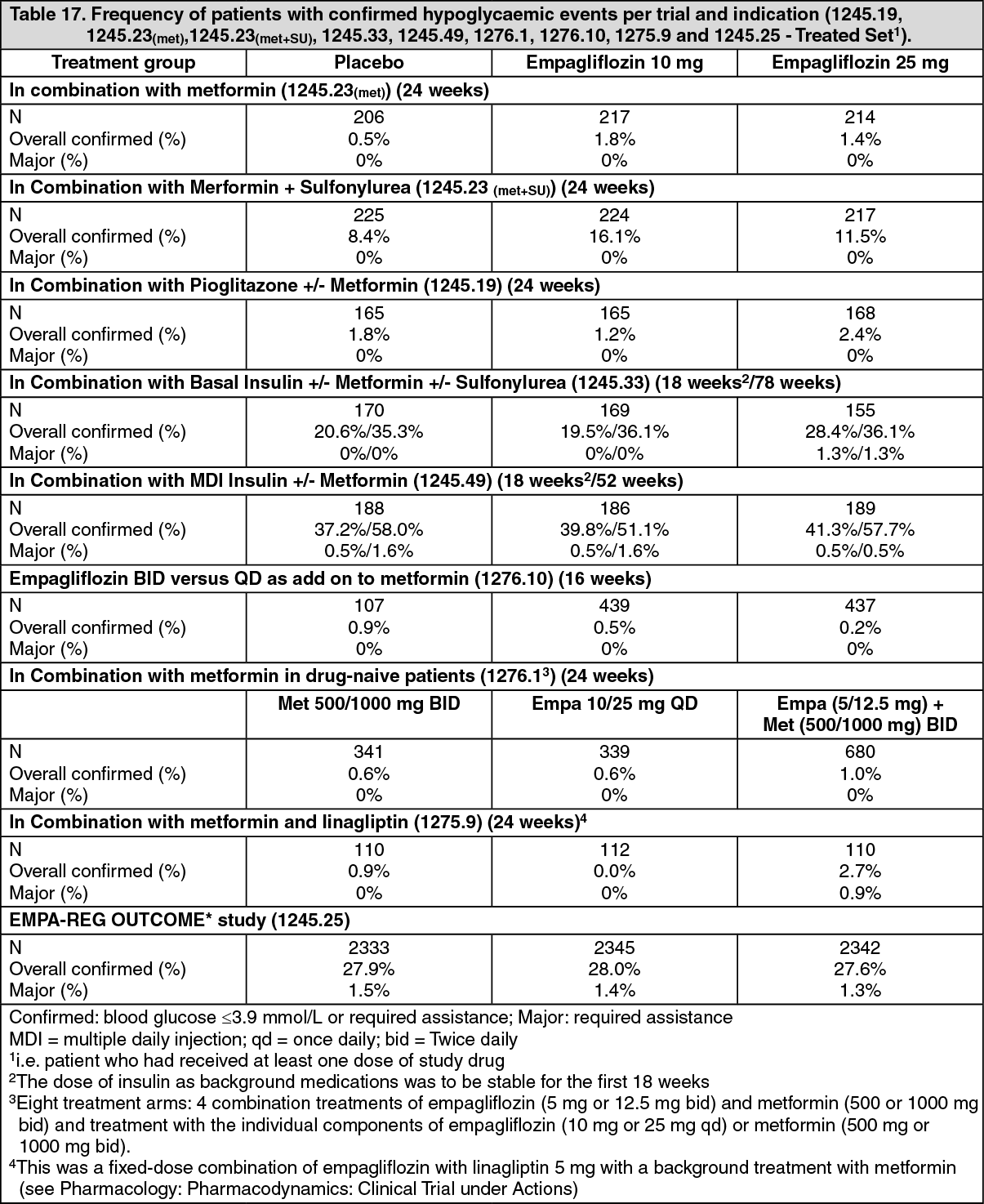
Hypoglycaemia: The frequency of hypoglycaemia depended on the background therapy in the respective studies and was similar to placebo for empagliflozin as add-on to metformin and as add-on to pioglitazone +/-metformin, and as add-on with linagliptin + metformin. The frequency of patients with hypoglycaemia was increased in patients treated with empagliflozin compared to placebo when given as add-on to metformin plus sulfonylurea, and as add-on to insulin +/- metformin and +/- sulfonylurea (Table 17).
Major hypoglycaemia (events requiring assistance): The overall frequency of patients with major hypoglycaemic events was low (<1%) and similar for empagliflozin and placebo on a background of metformin. The frequency of major hypoglycaemia depended on the background therapy in the respective studies. (See Dosage & Administration; see Table 17 as follows.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageUrinary tract infection: The overall frequency of urinary tract infection adverse events was higher in patients treated with empagliflozin 10 mg plus metformin (8.8%) as compared to empagliflozin 25 mg plus metformin (6.6%) or placebo plus metformin (7.8%). Similar to placebo, urinary tract infection was reported more frequently for empagliflozin plus metformin in patients with a history of chronic or recurrent urinary tract infections. The intensity of urinary tract infections was similar to placebo. Urinary tract infection events were reported more frequently for empagliflozin 10 mg plus metformin compared with placebo in female patients, but not for empagliflozin 25 mg plus metformin. The frequencies of urinary tract infections were low for male patients and were balanced across treatment groups.
Vaginal moniliasis, vulvovaginitis, balanitis and other genital infection: Vaginal moniliasis, vulvovaginitis, balanitis and other genital infections were reported more frequently for empagliflozin 10 mg plus metformin (4.0%) and empagliflozin 25 mg plus metformin (3.9%) compared to placebo plus metformin (1.3%), and were reported more frequently for empagliflozin plus metformin compared to placebo in female patients. The difference in frequency was less pronounced in male patients. Genital tract infections were mild and moderate in intensity, none was severe in intensity.
Increased urination: As expected via its mechanism of action, increased urination (as assessed by preferred term search including pollakiuria, polyuria, nocturia) was observed at higher frequencies in patients treated with empagliflozin 10 mg plus metformin (3.0%) and empagliflozin 25 mg plus metformin (2.9%) compared to placebo plus metformin (1.4%). Increased urination was mostly mild or moderate in intensity. The frequency of reported nocturia was comparable between placebo and empagliflozin, both on a background of metformin (<1%).
Volume depletion: The overall frequency of volume depletion [including the predefined terms blood pressure (ambulatory) decreased, blood pressure systolic decreased, dehydration, hypotension, hypovolaemia, orthostatic hypotension, and syncope] was low and comparable to placebo [empagliflozin 10 mg plus metformin (0.6%), empagliflozin 25 mg plus metformin (0.3%) and placebo plus metformin (0.1%)]. The effect of empagliflozin on urinary glucose excretion is associated with osmotic diuresis, which could affect the hydration status of patients age 75 years and older. In patients ≥75 years of age volume depletion events have been reported in a single patient treated with empagliflozin 25 mg plus metformin.
Blood creatinine increased and glomerular filtration rate decreased: The overall frequency of patients with increased blood creatinine and decreased glomerular filtration rate was similar between empagliflozin and placebo as add-on to metformin (blood creatinine increased: empagliflozin 10 mg 0.5%, empagliflozin 25 mg 0.1%, placebo 0.4%; glomerular filtration rate decreased: empagliflozin 10 mg 0.1%, empagliflozin 25 mg 0%, placebo 0.2%).
In these placebo-controlled, double-blind studies up to 24 weeks, initial transient increases in creatinine (mean change from baseline after 12 weeks: empagliflozin 10 mg 0.02 mg/dL, empagliflozin 25 mg 0.02 mg/dL) and initial transient decreases in estimated glomerular filtration rates (mean change from baseline after 12 weeks: empagliflozin 10 mg -1.46 mL/min/1.73m2, empagliflozin 25 mg -2.05 mL/min/1.73m2) have been observed. In the long term studies, these changes were generally reversible during continuous treatment or after drug discontinuation (see Figure 6 in Pharmacology: Pharmacodynamics: Clinical Trials under Actions for the eGFR course in the EMPA-REG OUTCOME study).
Laboratory parameters: Haematocrit increased: In a pooled safety analysis of all trials with metformin background treatment, mean changes from baseline in haematocrit were 3.6% and 4.0% for empagliflozin 10 mg and 25 mg, respectively, compared to 0% for placebo. In the EMPA-REG OUTCOME study, haematocrit values returned towards baseline values after a follow-up period of 30 days after treatment stop.
Serum lipids increased: In a pooled safety analysis of all trials with metformin background treatment, mean percent increases from baseline for empagliflozin 10 mg and 25 mg versus placebo, respectively, were total cholesterol 5.0% and 5.2% versus 3.7%; HDL-cholesterol 4.6% and 2.7% versus -0.5%; LDL-cholesterol 9.1% and 8.7% versus 7.8%; triglycerides 5.4% and 10.8% versus 12.1%.
View ADR Monitoring Form